January 11, 2019

11 Jan 2019
Rachel Ryan recently went to Baringo County, 370 km North West of Nairobi in Kenya to assist with the Franciscan Missionaries of St. Joseph, who have been operating a dispensary in Salawa for the past 28 years.
She sent us this report from her outreach visit with the mobile clinic on 23rd November, just over 2 weeks after her arrival in the country.
“On Friday the 23rd November I accompanied the mobile clinic to Lake Kamnorok Primary School. A distance of only 20 or so kilometers from Salawa, it still takes over an hour to get there due to the quality of the roads – which are in a far better state than they used to be, thanks to recent government investment. All the roads around Salawa are currently being levelled and surfaced with single membrane tarmacadam, and already the road from Salawa to Ajnamoi is paved with an initial layer, the surface still kicking up pieces of gravel, as we wait in joyful hope for another layer of tarmacadam. Anajmoi is the village just south of Salawa where the road splits to go towards Kabarnet in the East or Eldoret in the West. Our hope is sustained by the sections of road still closed off for surface work. At these sections, the traffic simply finds its own way round, veering off to parallel roadways of well packed dirt that have been carved out while the work is ongoing. So far these are fairly smooth and useable, though often, only one car wide, requiring some backtracking and maneuvering when one meets a truck coming fast in the opposite direction. My clinic colleagues tell me that outreach used to be much more of an ordeal when the roads were all mud and there were no bridges – a scant 6 months ago.

Outreach, or mobile clinic days, take place once a month for each outreach site. Lake Kamnorok is usually on the last Friday of the month but because of preparations for World Aids Day on the 1st December, this month it took place on the second last Friday. Most clinic staff start the day at 8:30am, so this is when the preparations for leaving began. The clinic’s driver, Jacob, had been on leave for some time and this was my first time meeting him. While others selected and laid out the equipment, supplies and boxes of medication that would be used during the day, Jacob was thoroughly checking the engine and undercarriage of our huge and faithful Toyota land-cruiser, which I have dubbed Big Bertha. Including the driver and myself, there were seven of us travelling – 3 nurses, a lab tech and our social worker.
Instead of coming out of the compound and going right and south towards Anamoj we went left and North towards the lake. At the far edge of Salawa village, we pulled into the Government clinic to collect more supplies. In theory, the Government clinic is better supplied than ours and open for 24 hour admission.
In practice, it’s hard enough to find someone to deal with during normal working hours and the service is perfunctory. After hours there is usually no one there.
Because the sisters live on-site at the clinic, people perceive Salawa PHC as a 24-hour facility and will come up and knock on the door of the house even if all the lights are off, and despite the large “working hours 8am to 5pm” sign over the clinic entrance.
Recently, a small maternity wing has been set up in one of the less-used outhouses, and so a system of night shift cover has been set up, but with a small staff there isn’t always someone available and if someone presents with a more challenging condition Head Nurse, Sr. Veronica may easily receive a late night call and end up working half the night.
Kerio valley is surprisingly populous and along the road we pass through many small villages and by many pedestrians, keeping to the verge, in the absence of anything resembling a footpath. Children who spotted me in the front cab, squashed beside Consolata, the social worker in the one-and-a-half passenger seat, waved enthusiastically and called out with the traditional Mzungu greeting: “How are you?” Towards the interior the houses we passed were traditionally made – what an Irish person might recognize as crannogs – low, round, clay walled houses with grass roofs.

I would imagine these are far more comfortable than the common village alternative of shanty houses, walled and roofed in corrugated tin. The crannogs at least offer some insulation, and sometimes the clay walls are decorated with swirls of colour or pale carvings. Combined with the brightly coloured washing out on lines or fences to dry, it was a very aesthetic sight. One photo I missed was the grass-roofed house with solar panels nestled in the thatch and a satellite aerial jutting from the join between wall and roof.
When we turned off towards the lake we lost the good road surface. Slowly, lurching over stony ruts and crevices, we passed water carriers with their pale, yellow jerry cans and negotiated our way through a small herd of cattle.
Our first stop was by the lake itself, in the peaceful woodland surrounding it, so we could have lunch. The lake was beautiful in its greenness. Apparently, in years gone by, it was a popular watering hole for elephants, and crocodiles still live in some muddy stretches. I resolved to avoid those but I did walk down to the waters edge reflecting once again on how much beauty there is on offer in this part of the world.
Lunch was githeri and chai for the rest of the staff, hard boiled eggs and sweet bananas for me (my travel diet of choice). Githeri is a staple meal of Kenya, which I find far more appealing than the maize-meal porridge of ugali, the staple diet throughout East Africa. For githeri corn kernels are cooked, long enough that they become swollen and soft as chickpeas, then mixed with cooked kidney beans. It’s plain but tasty. The chai is generally a weak tea that consists mainly of watered down milk, which is boiled at some length together with the tea leaves. Lunch was eaten and everyone washed up afterwards – with the water that had been carried along for that specific purpose.
It was about 12:30 at this stage and patients had gathered on the grounds of Lake Kamnorok primary school, a few hundred metres up the road from the water’s edge.
This is always the site for the mobile clinic. We set to unpacking boxes and people while Ken Kirop, one of the senior nurses, walked the grounds and returned to discuss options for setting up stations. There would be four areas – one for outpatients, one for the weighing / growth monitoring of babies, one for immunization and one for antenatal care.
Ken and Fred Serem, the lab technician, each addressed the waiting patients, both able to speak the local language as well as Kiswahili. These short talks often address some health issue or point of advice and are generally an opportunity to thank patients for attending the clinic, advising them when to seek medical advise and urging mothers to pay attention to the growth monitoring results for the health and development of their children. They also simply introduce the format of the day and layout of the stations. Today, they also introduced me, explaining that I was mostly there to observe the work of the staff and that I may take a few photos – but that they were free to object to this at any time, and not have their photo taken. During the day one man and one teenage girl asked that their photos not be taken, but by and large people were happy with it. After I delivered a simple smile and wave greeting, I took a couple of group photos, and then the patients split into the various groups. It became immediately obvious that the weighing station would be the busiest – and so it remained throughout the day.
I moved from station to station, asking about common ailments and treatments, but I was brought back again and again to Growth Monitoring, since they were constantly swamped with people. Our driver had immediately positioned himself to help, which I learned was normal on these outreach sessions.
He started taking the height measurement of the babies and measurement of mid upper arm circumference (MUAC), which is a standard rule of thumb for nutritional monitoring. Social worker, Consolata did the weights and the bookkeeping.
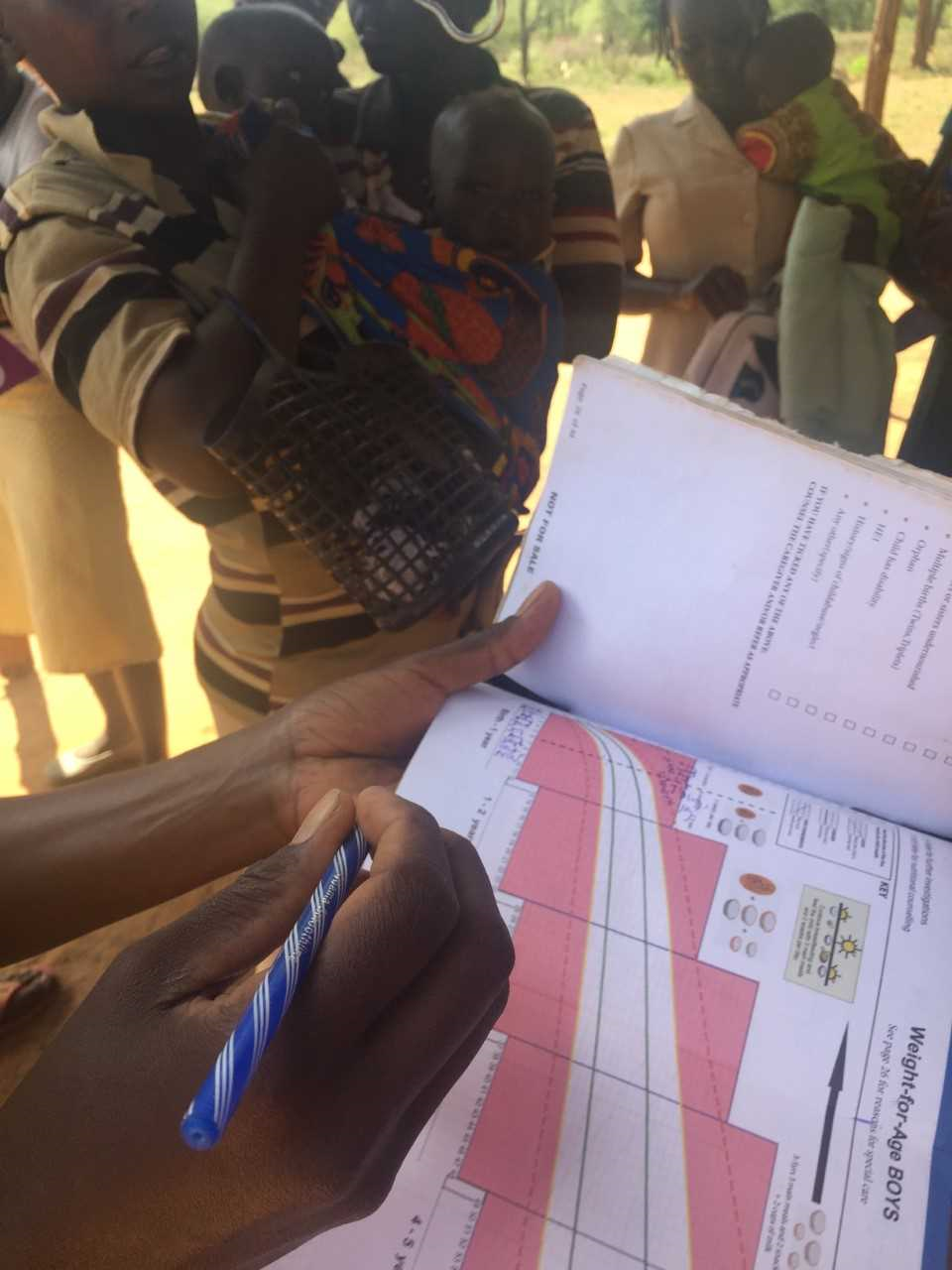
When a pregnant woman first presents herself to any health facility she is given a Mother and Child Health Handbook, in which, among other things, she is encouraged to track the growth development of her baby as well as record the vaccinations they receive. So, each measurement must be recorded in the mother’s book, along with the patient details. The corresponding record must be recorded in the Ministry of Health Patient Register, required by every facility. If the mother requires any additional or supplemental treatment such as Vitamin A or De-worming tablets, she will also pay for it at this time and be provided with a written receipt.
The scales and height board are brought in by the staff, the weighing scales is tied to any available cross beam with strong rope. Babies are generally tied to their mothers’ backs with a large swathe of cloth they call a “lasso” in this context. When they are called forward for the weighing, the mother will simply swing the baby round in front of them and pass the knotted cloth over their heads. The baby can then be easily hung from this functional sling. Given the physical work required to weigh and measure each child, and the administrative records required, it seemed impossible that two people could process twenty patients in two hours, let alone two or three times that, without a great deal of error and confusion. Certainly, there was an air of frenetic intensity in the work being carried out, but Consolata and Jacob proceeded with a systematic focus, born of long practice. I was willingly roped in to help with the recording of data, scribbling weights and measurements on mothers’ handbooks as they were called out and learning where to put the information required for the patient register books. Any time I left to see another station I felt a strong pang of guilt, since no other station was as busy as this particular one.
The vaccination station, manned by Ken, was set up around the corner from Growth Monitoring, for the convenience of the mothers, and I didn’t stay there for any length of time. It seemed cruel to compound the unhappiness of a child in pain with an audience. The mandatory vaccinations include TB, polio, whooping cough, diphtheria, measles, hepatitis b and yellow fever, and all doses should be delivered before the child turns two.
The schedule for these vaccinations is kept in the mothers’ handbook and health workers write in the dates for any follow-up required. At the outpatient station, a steady line of patients presented with various ailments for our nurse, Joan. Most were sent on to visit Fred, who had set up his lab, as usual, for outreach days, in the back of Big Bertha. Many common conditions can be screened for by a simple blood test, including malaria, hepatitis, typhoid and brucella. They will also often perform a pregnancy test, since some treatments are contra indicated for pregnant mothers – especially doxycycline for brucella. Fred sat in one of the two back seats, with sample kits and equipment on the other seat and test tubes lined up on Big Bertha’s spare tyre. beside him. Patients squished in with him which meant that at least they had the benefit of shade and privacy.
For the antenatal station, nurse, Juliette had set up in one of the school classrooms and a privacy curtain divided the patient’s bed – a folding bed brought in with the rest of the equipment – from the desk and two chairs where people could consult. Basic tests there included blood pressure, anaemia and foetal heartbeat as well as palpitations to check the baby’s head and position.
As the number of patients to be seen wore down, the Growth Monitoring station ended up with a stack of pink health handbooks, as transcription of full details into Ministry of Health Child Welfare Clinic Register lagged (understandably) behind. I joined in this effort and passed the books to Consolata as I was done.
The mothers stood around, patiently, with babes in arms and some by the hand, waiting for one or other of us to call their child’s name and retrieve their books. When they had it back and were done for the day, the women and children retreated to the shade, at the edge of the school’s compound, where other mothers, patients and companions had set up blankets and cooking equipment. Some had brought fruit to distribute or to sell – to each other and to us. Some of the nurses bought tomatoes or pawpaw for their evening meal, even while we were packing up the land-cruiser.
Somehow, everything had taken place in less than 5 hours. More than 60 patients had been seen, more than 40 of them in the Growth Monitoring section. My colleagues informed me that this was a very quiet day – perhaps because we had come a week early or perhaps because a government clinic had recently opened in a neighbouring village. Attendance at the mobile clinics is always monitored, to be sure we are making best use of our resources. We arrived back to Salawa PHC at 18.30 and unpacked everything. I was tired, but had enjoyed spending the day directly engaged with the patients, rather than closed away in an administrative office. It was gratifying to see the appreciation of the people, on the ground, and the professionalism of our staff. It is always good to know that you are needed.”